Vorasidenib
My tumor has IDH1 R132C. That is why IDH inhibition matters here. Vorasidenib is FDA-approved for grade 2 astrocytoma or oligodendroglioma with a susceptible IDH1 or IDH2 mutation after surgery, and it is the IDH inhibitor I am on now.
This is how I currently understand the biology of my tumor, what looks promising, what is still uncertain, and how the vaccine idea fits into the larger treatment story.
What I am trying to do is go after the tumor in two different ways: use an FDA-approved IDH inhibitor for the mutation that defines my cancer, and explore a personalized vaccine that tries to make selected tumor mutations visible to my immune system. This is my treatment story, not proof that the vaccine, or the combination, improves outcomes.
My tumor has IDH1 R132C. That is why IDH inhibition matters here. Vorasidenib is FDA-approved for grade 2 astrocytoma or oligodendroglioma with a susceptible IDH1 or IDH2 mutation after surgery, and it is the IDH inhibitor I am on now.
The vaccine is exploratory and personal to my tumor. The combination with IDH inhibition is exploratory too. It uses mutation-spanning peptides, with the goal of helping T cells notice pieces of the cancer that should not exist in normal tissue.
I want this page to work less like a polished conclusion and more like a map of the case: what was measured, what I generated, what is public here, and what still needs source reports or direct access.
Diagnosis, surgery, surveillance, treatment starts, vaccine milestones, and the life around all of it.
OverviewDiagnosis, IDH inhibitor context, somatic calls, peptide funnel counts, TMB/MSI, purity, and PGx coverage.
Vaccine funnelHow my tumor mutations became a computational peptide list, then a smaller vaccine-design shortlist.
Variant atlasIDH1, ATRX, TP53 / Li-Fraumeni context, MGMT methylation, HLA type, and vaccine-relevant peptides.
Raw accessRaw genome, tumor VCF, peptide-level files, and source reports need privacy boundaries and version notes.
These are the numbers I keep coming back to. Some come directly from my medical reports. Some are first-pass counts from the tools I built to understand the case.
I worked with a pipeline that starts with mutations in my tumor and narrows them down to peptides most likely to be visible to my immune system. Those peptides then become the starting point for a personalized vaccine.
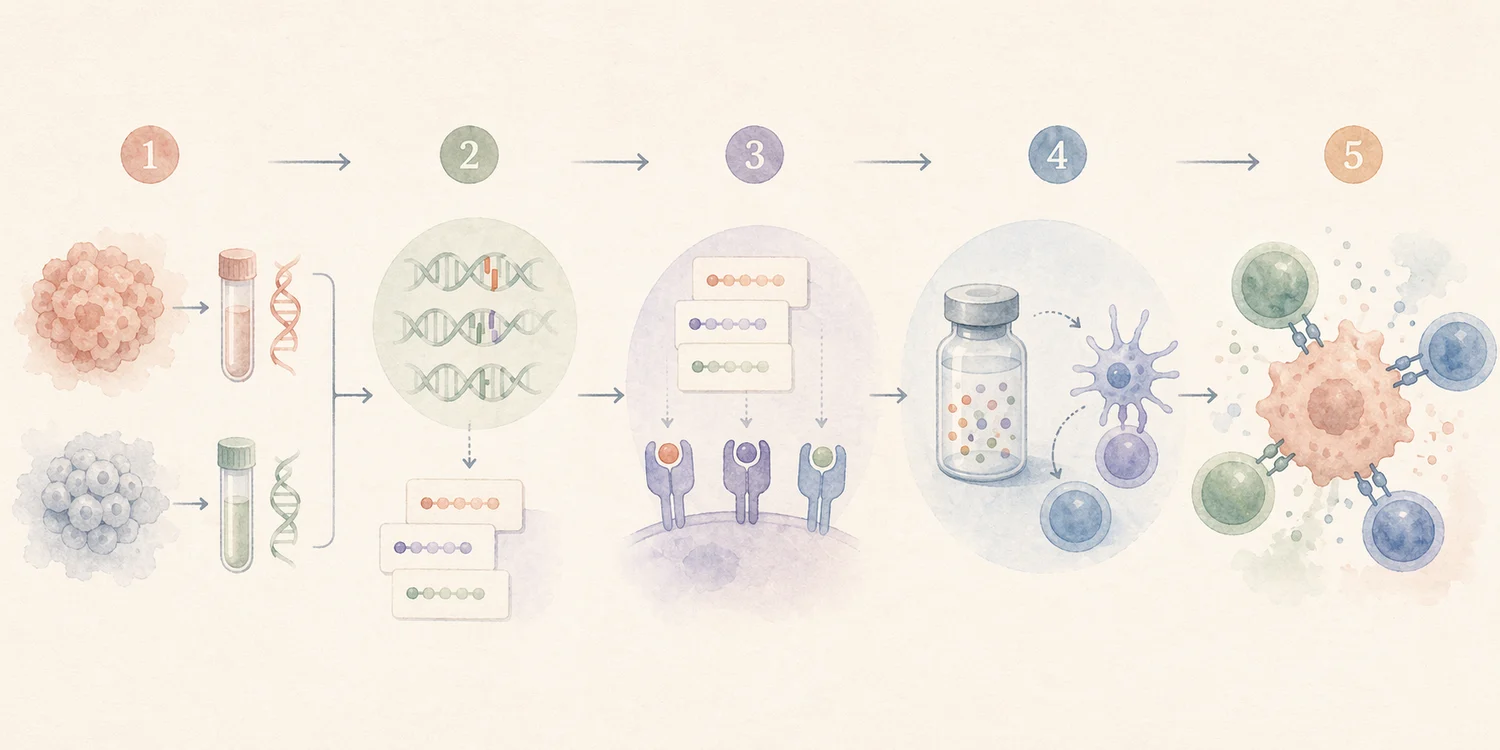
Find mutations that are present in the cancer and different from normal tissue.
Look for mutation-spanning peptides that could be shown by my HLA molecules.
Use selected peptides as patient-specific vaccine material.
The goal is for immune cells to recognize selected pieces of the tumor.
Start with tumor sequencing and look for mutation-spanning peptides that should look different from normal self.
CeGAT's vaccine is personalized rather than off-the-shelf: the input is my tumor's molecular profile.
The point is to help T cells recognize a patient-specific tumor profile, using peptides selected from the tumor's own mutations.
These are the core tumor findings and vaccine-relevant signals I am sharing from my Tempus, BostonGene, pathology, and report data.
If this story makes you want to help, these are established places to support brain tumor research, patient programs, and translational work.
Research funding, patient education, and support for people facing brain tumors.
National advocacyResearch, policy work, and patient-centered advocacy across brain tumor types.
Academic centerClinical and translational brain tumor research at UCSF.
Translational researchEarly-phase research and trials focused on brain tumor treatment.
Research nonprofitResearch support focused on glioblastoma and aggressive brain tumors.
Research foundationFunding and programs for brain cancer research and early-career investigators.